A Patient's Guide to Cubital Tunnel Syndrome
Introduction
Cubital tunnel syndrome is a condition that affects the ulnar nerve where it crosses the inside edge of the elbow. The symptoms are very similar to the pain that comes from hitting your funny bone. When you hit your funny bone, you are actually hitting the ulnar nerve on the inside of the elbow. There, the nerve runs through a passage called the cubital tunnel. When this area becomes irritated from injury or pressure, it can lead to cubital tunnel syndrome.
This guide will help you understand
- what causes this condition
- ways to make the pain go away
- what you can do to prevent future problems
Anatomy
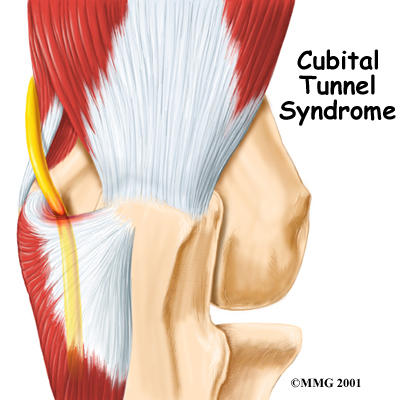
What is the cubital tunnel?
The ulnar nerve actually starts at the side of the neck, where the individual nerve roots leave the spine. The nerve roots exit through small openings between the vertebrae. These openings are called neural foramina.
The nerve roots join together to form three main nerves that travel down the arm to the hand. One of these nerves is the ulnar nerve.
The ulnar nerve passes through the cubital tunnel just behind the inside edge of the elbow. The tunnel is formed by muscle, ligament, and bone. You may be able to feel it if you straighten your arm out and rub the groove on the inside edge of your elbow.
The ulnar nerve passes through the cubital tunnel and winds its way down the forearm and into the hand. It supplies feeling to the little finger and half the ring finger. It works the muscle that pulls the thumb into the palm of the hand, and it controls the small muscles ( intrinsics) of the hand.
Causes
What causes cubital tunnel syndrome?
Cubital tunnel syndrome has several possible causes. Part of the problem may lie in the way the elbow works. The ulnar nerve actually stretches several millimeters when the elbow is bent. Sometimes the nerve will shift or even snap over the bony medial epicondyle . (The medial epicondyle is the bony point on the inside edge of the elbow.) Over time, this can cause irritation.
One common cause of problems is frequent bending of the elbow, such as pulling levers, reaching, or lifting. Constant direct pressure on the elbow over time may also lead to cubital tunnel syndrome. The nerve can be irritated from leaning on the elbow while you sit at a desk or from using the elbow rest during a long drive or while running machinery. The ulnar nerve can also be damaged from a blow to the cubital tunnel.
Symptoms
What does cubital tunnel syndrome feel like?
Numbness on the inside of the hand and in the ring and little fingers is an early sign of cubital tunnel syndrome. The numbness may develop into pain. The numbness is often felt when the elbows are bent for long periods, such as when talking on the phone or while sleeping. The hand and thumb may also become clumsy as the muscles become affected.
Tapping or bumping the nerve in the cubital tunnel will cause an electric shock sensation down to the little finger. This is called Tinel's sign.

Diagnosis
How will my doctor know I have cubital tunnel syndrome?
Your doctor will take a detailed medical history. You will be asked questions about which fingers are affected and whether or not your hand is weak. You will also be asked about your work and home activities and any past injuries to your elbow.
Your doctor will then do a physical exam. The cubital tunnel is only one of several spots where the ulnar nerve can get pinched. Your doctor will try to find the exact spot that is causing your symptoms. The prodding may hurt, but it is very important to pinpoint the area causing you trouble.
You may need to do special tests to get more information about the nerve. One common test is the nerve conduction velocity (NCV) test. The NCV test measures the speed of the impulses traveling along the nerve. Impulses are slowed when the nerve is compressed or constricted.
The NCV test is sometimes combined with an electromyogram (EMG). The EMG tests the muscles of the forearm that are controlled by the ulnar nerve to see whether the muscles are working properly. If they aren't, it may be because the nerve is not working well.
Treatment
How can I make my pain go away?
Nonsurgical Treatment
The early symptoms of cubital tunnel syndrome usually lessen if you just stop whatever is causing the symptoms. Anti-inflammatory medications may help control the symptoms. However, it is much more important to stop doing whatever is causing the pain in the first place. Limit the amount of time you do tasks that require a lot of bending in the elbow. Take frequent breaks. If necessary, work with your supervisor to modify your job activities.
If your symptoms are worse at night, a lightweight plastic arm splint or athletic elbow pad may be worn while you sleep to limit movement and ease irritation. Wear it with the pad in the bend of the elbow to keep the elbow straight while you sleep. You can also wear the elbow pad during the day to protect the nerve from the direct pressure of leaning.
Doctors commonly have their patients with cubital tunnel syndrome work with a physical or occupational therapist. At first, your therapist will give you tips how to rest your elbow and how to do your activities without putting extra strain on your elbow. Your therapist may apply heat or other treatments to ease pain. Exercises are used to gradually stretch and strengthen the forearm muscles.
Surgery
Your symptoms may not go away, even with changes in your activities and nonsurgical treatments. In that case, your doctor may recommend surgery to stop damage to the ulnar nerve.

The goal of surgery is to release the pressure on the ulnar nerve where it passes through the cubital tunnel. There are two different kinds of surgery for cubital tunnel syndrome. It is not clear whether one operation is better than the other.
Ulnar Nerve Transposition
One method is called >ulnar nerve transposition. In this procedure, the surgeon forms a completely new tunnel from the flexor muscles of the forearm. The ulnar nerve is then moved (transposed ) out of the cubital tunnel and placed in the new tunnel.
Medial Epicondylectomy
The other method simply removes the medial epicondyle on the inside edge of the elbow, a procedure called medial epicondylectomy . By getting the medial epicondyle out of the way, the ulnar nerve can then slide through the cubital tunnel without pressure from the bony bump.
Cubital tunnel surgery is often done as an outpatient procedure. This means you won't have to stay in the hospital overnight. Surgery can be done using a general anesthetic, which puts you to sleep, or a regional anesthetic. A regional anesthetic blocks the nerves in only one part of your body. In this case, you would have an axillary block , which would affect only the nerves of the arm.
Rehabilitation
What can I expect after treatment?
Nonsurgical Rehabilitation
If nonsurgical treatments are successful, you may see improvement in four to six weeks. Your physical or occupational therapist works with you to ease symptoms and improve elbow function. Special exercises may be used to help the ulnar nerve glide within the cubital tunnel. Treatment progresses to include strengthening exercises that mimic daily and work activities.
You may need to continue wearing your elbow pad or splint at night to control symptoms. Try to do your activities using healthy body and wrist alignment. Limit repeated motions of the arm and hand, and avoid positions and activities where the elbow is held in a bent position.
After Surgery
Recovery after elbow surgery depends on the procedure used by your surgeon. If you only had the medial epicondyle removed, you'll have a soft bandage wrapped over your elbow after surgery. Therapy can progress quickly after this type of surgery. Treatments start out with range-of-motion exercises and gradually work into active stretching and strengthening. You just need to be careful to avoid doing too much, too quickly.
Therapy goes slower after ulnar nerve transposition surgery. You could require therapy for three months. This is because the flexor muscles had to be sewn together to form the new tunnel. Your elbow will be placed in a splint and wrapped in bulky dressing, and your elbow will be immobilized for three weeks.
When the splint is removed, therapy will begin with passive movements. In passive exercises, your elbow is moved, but your muscles stay relaxed. Your therapist gently moves your arm and gradually stretches your wrist and elbow. You may be taught how to do passive exercises at home.
Active therapy starts six weeks after surgery. You begin to use your own muscle power in active range-of-motion exercises. Light isometric strengthening exercises are started. You may begin careful strengthening of your hand and forearm by squeezing and stretching special putty. These exercises work the muscles without straining the healing tissues.
At about eight weeks, you'll start doing more active strengthening. Your therapist will give you exercises to help strengthen and stabilize the muscles and joints in the wrist, elbow, and shoulder. Other exercises are used to improve fine motor control and dexterity of the hand.
Some of the exercises you'll do are designed get your elbow working in ways that are similar to your work tasks and sport activities. Your therapist will help you find ways to do your tasks that don't put too much stress on your elbow. Before your therapy sessions end, your therapist will teach you a number of ways to avoid future problems.
You will need the Adobe Reader to view and print these documents. 
*Disclaimer:* The information contained herein is compiled from a variety of sources. It may not be complete or timely. It does not cover all diseases, physical conditions, ailments or treatments. The information should NOT be used in place of visit with your healthcare provider, nor should you disregard the advice of your health care provider because of any information you read in this topic.